Anterior resection
This page gives you information about the procedure known as an anterior resection. It explains what the procedure involves and also some of the common complications related with it.
On this page
-
The digestive system
-
What is an anterior resection?
-
Will I need a stoma?
-
What is keyhole surgery?
-
Potential risks and complications of the surgery
-
What are the benefits of the procedure?
-
Alternative treatments
-
How long does the operation take?
-
How long will I be in hospital?
-
If you have a stoma
-
Pre-operative, post-operative and discharge advice
-
Results (if your operation has been performed to remove a cancer)
-
Follow-up
-
Contact information
-
Further information
The digestive system
To help you understand your operation, it is helpful to have a basic knowledge of how the body works (see Figure 1).
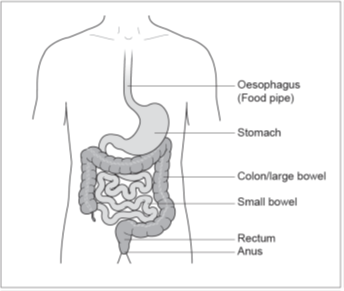
When food is eaten, it passes from the mouth down the oesophagus (food pipe) and into the stomach.
The food is broken down and becomes semi-liquid. It then continues through the intestine (small bowel), which is many feet long, where food is digested and the nutrients are absorbed.
The semi-liquid food then passes into the colon (large bowel) where it becomes faeces (stools). The main job of the colon is to absorb water into our bodies making the stools more solid.
The stools then enter a storage area called the rectum. When the rectum is full, we get the urge to open our bowels. The stools are finally passed through the anus (back passage) when we go to the toilet.
What is an anterior resection?
An anterior resection is an operation to remove the area of your bowel that is diseased. In this case part or all of your rectum will be removed. Your consultant or colorectal nurse specialist will discuss this with you in more detail with the aid of a diagram (Figure 2) which shows you which part of the bowel may be removed.
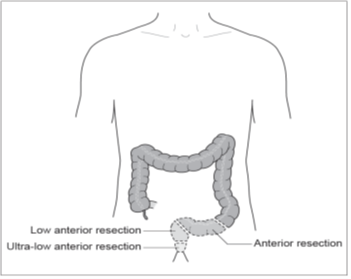
A cut will be made in your abdomen (tummy) and the surgeon will remove the diseased area of bowel. The two healthy ends of the bowel are then joined by stitching or stapling them together (anastomosis). The wound on the abdomen is usually closed with dissolvable stitches.
Will I need a stoma?
It may be necessary to have a temporary stoma to divert stools away from the surgical join in the bowel while it heals. If this is the case, part of the small bowel would be brought out onto the surface of the abdominal wall to form an ileostomy. Stools are then passed through the stoma and collected in a bag.
Your surgeon will discuss with you your individual risk of having a stoma formed.
Before your operation, a stoma nurse will mark your abdomen (known as a siting) with a skin marker pen. This is to guide your surgeon to the best possible place to bring out the stoma if it is necessary. Your stoma nurse will also discuss with you, in more detail, what having a stoma will involve and answer any questions you may have.
If you do require a stoma, a second smaller operation to reverse the stoma may be performed so that your stools pass through your anus (back passage) in the normal way again. Before this can be done it would be necessary to check that the join in your bowel has fully healed with a special X-ray. The timing of this operation will be discussed with you by your consultant and colorectal nurse specialist but is usually done a few months after the first operation. If you have any treatment after your operation, for example chemotherapy, the stoma would normally be reversed after your treatment has finished.
Before your operation, your consultant surgeon and colorectal and stoma care nurse specialist will carefully explain the procedure involved. You will be asked to sign a consent form to confirm that you understand and agree to have the surgery.
The surgery may either be done as an ‘open’ operation which involves making a large cut in the abdomen, or using laparoscopic (keyhole) surgery.
What is keyhole surgery?
Keyhole surgery involves carrying out an operation through small cuts in the abdomen. The surgeon inserts a narrow telescope attached to a camera and other specialist instruments through the cuts to remove the affected part of bowel. Most of the operation is made through these cuts, but a slightly larger opening is needed to remove the section of bowel from the body (this is usually a bikini line cut).
The decision about whether to use open or keyhole surgery should be made after an informed discussion between you and your surgeon. In particular, your surgeon has to consider whether your condition is suitable for keyhole surgery and the risks and benefits of both procedures.
The benefits of keyhole surgery include:
- A reduction in the length of your hospital stay
- Reduced discomfort following the surgery
- A smaller scar
The risks associated with keyhole surgery are the same as for open surgery. If for technical reasons it is not possible to complete your operation using keyhole surgery then the surgeon would need to proceed to an open operation. This will be discussed with you during the consent process.
Potential risks and complications of the surgery
Removing part of the bowel is a major operation. Risks with this operation include:
Anastomotic leak
Sometimes the anastomosis (join in the bowel) leaks. Treatment with antibiotics and resting the bowel are generally enough. However, this may be a serious complication which needs further surgery and formation of a stoma.
Nerve damage
The piece of bowel operated on is very close to the bladder and the nerves responsible for sexual function. These nerves may get damaged during the operation. Bladder function may also be disturbed.
Men may experience difficulty with erection and ejaculation and some may have problems passing urine.
Women may feel a different sensation in their vagina when having intercourse. There may be pain, vaginal tenderness, dryness or vaginal discharge for some months.
These complications may be temporary but can be permanent. If you experience any of these problems after your operation, please discuss them with your surgeon or colorectal nurse specialist as there may be treatments available to help.
Ileus (paralysis of the bowel)
Sometimes the bowel is slow to start working after surgery.
This causes vomiting and delays you from eating and drinking normally. If this happens, the bowel may need to be rested and a drip (a tube into a vein in your arm) is used to give you fluids (instead of drinking). In addition, you may also need a nasogastric tube (tube in your nose which passes into your stomach) so that fluid collecting in your stomach can be drawn off. This will help to prevent nausea and vomiting and will remain in place until the bowel recovers.
Stoma problems
- A necrotic stoma (reduced blood supply to the stoma). This may need further surgery.
- Stoma prolapse (when the stoma comes out too far past the skin). In serious cases further surgery may be needed.
- Parastomal hernia (when the bowel pushes through a weak point in the abdominal muscle wall). Small hernias can be treated with a support garment or belt. Surgery may be needed for larger hernias.
Bowel function
Problems with bowel function may happen after surgery or after your ileostomy has been reversed.
Different bowel patterns are experienced and you may have any of the following:
- Frequency of stool
- Urgency of stool
- Diarrhoea
- Fragmentation of stool (this is when you need to visit the toilet often and can pass only small amounts of stool)
Bowel patterns are a very individual thing and therefore it is difficult to predict what your bowel pattern will be like. The bowel pattern usually settles quickly (in a matter of months) but it can take up to 2 years before you have a regular pattern.
Your consultant or colorectal nurse specialist will be able to give you individual advice if you experience any of the problems described in this section.
Adhesions (scar tissue)
With any abdominal surgery, there will be some formation of scar tissue. This is known as adhesions. In some people, this can lead to further problems which may require more surgery, but this is rare.
Pressure ulcers
Pressure ulcers, also known as pressure sores are caused by a combination of pressure, shearing and friction to the skin.
The nurses looking after you will assess your risk of developing a pressure ulcer daily, and will check your pressure areas regularly. You will be encouraged to change your position at regular intervals for pressure area relief. You will be assisted by your nursing staff if you need help to move.
Chest infection
You can help reduce the risk of a chest infection by practising regular deep breathing exercises and following the instructions of the physiotherapist.
If you smoke, we strongly advise you to stop.
Wound infection
If your wound becomes infected, this is usually not serious but may require treatment. You may be given antibiotics or if there is a collection of fluid, this may need to be released to allow your wound to continue to heal.
Thrombosis (blood clot in the leg)
Major surgery carries a risk of blood clot formation in the legs. To reduce this risk, a small dose of blood thinning medication will be given once a day by injection until you go home. It is likely that you will need to continue these injections for a short period of time at home. The nurse on the ward will help to train you so that you are able to do this safely or provide alternative arrangements with the community nursing team, if needed. You will also be fitted with some support stockings to be worn during your hospital stay. You can help to reduce the risk of blood clots forming by moving around as much as you are able to and particularly by exercising your legs.
Pulmonary embolism (blood clot in the lung)
Rarely, a blood clot from the leg can break off and become lodged in the lungs. This would need treatment with blood thinning medication.
Bleeding
A blood transfusion may be needed during or after your operation. Very rarely, further surgery may be required if there is continued bleeding after your operation.
Risk to life
Surgery to remove part of the bowel is classified as major surgery. It can carry a risk to your life. Your surgeon will discuss this risk with you.
Most people will not experience any serious complications from their surgery. However, risks do increase with age and for those who already have heart, chest, or other medical conditions such as diabetes or for those who are overweight or smoke.
What are the benefits of the procedure?
The operation aims to remove the diseased bowel. In most cases this will give you the best chance of a cure or significant improvement in your bowel problems.
Alternative treatments
If an anterior resection has been recommended by your surgeon as the best treatment option, not having this surgery may lead to bleeding, rectal discharge or incontinence, pain and possibly a complete blockage of the bowel. If you have cancer, the longer it remains the more likely it is to spread and become incurable. If you choose not to have surgery, radiotherapy and/or chemotherapy may be offered. This may control your symptoms but will not cure the disease.
Occasionally, it is possible to remove a rectal cancer using surgery directly from within the back passage. This type of surgery is only suitable for a small number of patients.
Another option is a stent which is a flexible hollow tube. A stent can be rolled up tightly so that it can be passed through the tumour or blockage. Once in place stents are able to expand to keep the bowel open and prevent a blockage.
This may help with symptoms but will not cure the disease.
Your surgeon will discuss these options if appropriate.
How long does the operation take?
This operation takes between 2 and 4 hours, however you will be off the ward for longer than this because of the time spent in the anaesthetic room before your operation and time in the recovery room afterwards. When you are fully awake after your anaesthetic, feeling comfortable and your general condition is stable, you will be taken back to the ward.
How long will I be in hospital?
During your admission, you will be following an enhanced recovery programme which aims to help you recover quickly and safely. We would estimate that you should be ready for discharge within 5 to 7 days if your recovery is uncomplicated and you are able to cope with your stoma.
If you have a stoma
The faeces (stool/poo) may start being passed directly into the pouch (bag) within 24 to 48 hours, but can take longer. When faeces first pass into the pouch, it will be liquid, this is normal. You will have a pouch over your stoma that can be emptied regularly. As you start to eat and drink a little more and build up your appetite, the faeces will thicken up to a ‘porridge like’ consistency.
By the time you go home, you will need to empty your stoma pouch on average 4 to 5 times per day down the toilet. Between the stoma nurse specialist and the ward nurses, they will show you on a daily basis what to do with your stoma. By the time you go home, you will know how to empty and change your stoma bag. It will feel fiddly at first but the more you do it, the easier it will get.
Even if you have a stoma, it is quite normal for you to pass a little old blood, faeces, stool, poo, mucus or wind from your back passage (bottom). You still have healthy bowel attached from the stoma down to your bottom. This healthy bowel naturally makes mucus and you will occasionally experience the need to open your bowels. Just sit on the toilet, relax and it will pass into the toilet.
Pre-operative, post-operative and discharge advice
For further information about what to expect when you come into hospital, what your recovery will involve and for discharge advice, please refer to leaflet GHPI0815 ‘Enhanced recovery programme for colorectal surgery’. You should be given a leaflet by your colorectal nurse specialist before your surgery.
Before your operation, your consultant surgeon and a colorectal and stoma care nurse specialist will carefully explain the procedure involved. You will be asked to sign a consent form to confirm that you understand and agree to have the surgery.
The surgery may either be done as an ‘open’ operation which involves making a large cut in the abdomen, or using laparoscopic (keyhole) surgery.
Results (if your operation has been performed to remove a cancer)
During your operation, the bowel and surrounding tissue that is removed will be sent to the pathology laboratory for analysis (investigation). The analysis process is very detailed and it will take about 7 to 10 days for the results to return. These results will then be discussed at a colorectal multidisciplinary team meeting. At this meeting, a consultant histopathologist will discuss the stage of your tumour in detail.
The stage is a term used to describe the extent of the cancer in the body. A joint decision between the specialists will then be made about whether or not further treatment should be recommended for you, such as chemotherapy or radiotherapy.
The multidisciplinary team will include:
- Colorectal consultant surgeons
- Clinical consultant oncologists
- Consultant radiologists
- Consultant pathologists
- Colorectal clinical nurse specialists
- Other specialists such as stoma nurses, the palliative care team, consultant gastroenterologists
Depending on your wishes, you can either be informed about your histology results by a telephone call from your specialist nurse or at an outpatient appointment with your consultant or specialist nurse.
Follow-up
Once you are discharged, your colorectal nurse specialist will make telephone contact to assess your general well-being within 24 to 48 hours. Alternatively, they will provide details while you are in hospital as to who you can contact if you have any concerns.
You will be seen for an outpatient appointment about 6 weeks following your discharge. You will either be seen by your consultant or one of the colorectal nurse specialists who will assess how well you are recovering from your operation and check your wounds.
If your operation was performed for cancer and you have requested to receive your results in clinic, then you may be seen 2 weeks following your discharge. Your consultant or colorectal nurse specialist will also discuss with you, your individualised follow up programme.
After discharge the stoma nurse specialist will telephone you to arrange a visit to your home or to see you in an outpatient clinic to check the stoma.
Contact information
Colorectal Nurse Specialist
Gloucestershire Royal Hospital
Tel: 0300 422 5617
Monday to Friday, 8:00am to 4:00pm
Outside of these hours, please leave a message and someone will return your call the next working day.
Stoma Nurse Specialist
Cheltenham General Hospital
Tel: 0300 422 4363
Monday to Friday, 8:00am to 4:00pm
Gloucestershire Royal Hospital
Tel: 0300 422 6702
Monday to Friday, 8:00am to 4:00pm
Outside of these hours, please leave a message and someone will return your call the next working day.
If you have an urgent problem, the stoma nurses can be contacted via the hospital switchboard.
Hospital Switchboard
Tel: 0300 422 2222
When prompted, ask for the operator then for the stoma nurses.
Further information
Macmillan Cancer Support
Tel: 0808 808 00 00
Monday to Friday, 9:00am to 8:00pm
Website: www.macmillan.org.uk
Bowel Cancer UK
Website: www.bowelcanceruk.org.uk
FOCUS Cancer Information Centre
Cheltenham General Hospital
Tel: 0300 422 4414
Monday to Friday, 8:30am to 4:30pm
Maggie’s Centre
College Baths Road, Cheltenham
Tel: 01242 250 611
Monday to Friday, 9:00am to 5:00pm
‘Mini’ Maggies
The Main Place, Old Station Way, Coleford GL16 8RH
Tel: 01242 250611
Offering practical and emotional support, facilitated and peer support groups as well as fitness and relaxation classes. Sessions run on the third Friday of each month from 10:00 am to 2:00 pm.
Macmillan Information Hub
Gloucestershire Royal Hospital
To access the service either drop in (no appointment needed) or:
Tel: 0300 422 8880
Monday to Friday, 9:00 am to 4:00pm
Email: ghn-tr.macmillanhub@nhs.net